
This is probably one of the most frequently asked questions regarding facelifts. There are so many different names used to describe facelifts that it can get confusing very quickly. In reality, all these different names refer to more often than not a very similar technique and sometimes a particular name is used not to differentiate a technique but rather to market a certain practice. A typical example is the so called “Lifestyle Lift” which did not refer to any particular technique but rather to a company that would attract business to its contracted surgeons by promoting the name. As for the bona fide techniques, the list below will attempt to clarify them.
Mini Face lift
a.k.a Mini Lift, S-Lift, Short Scar Facelift

- IncisionThe Mini Face lift provides a complete natural facelift with minimal incisions. The incision that is omitted is the submental incision or the one under the chin. As for the incisions around the ear, these can be limited to just in front of the ear, extending it to behind the ear. If the scar is extended further into the hairline behind the ear, the incision is no longer considered minimal and the technique starts resembling a full facelift.
- Skin-OnlyThe most basic Mini Lift technique is to make the incision and then remove skin in the area in front of the ear and close the incision. This technique is indicated in the younger cohort of patients desiring facial rejuvenation. The improvement can be subtle and does not last as long as other techniques. Its draw is that it can be performed quickly under local anesthesia in the office setting. However, for the incision used, it is probably better to perform a more sophisticated lift to the improve longevity of the result.
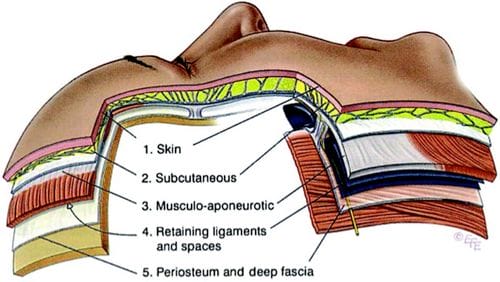
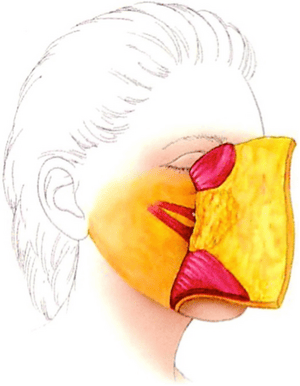
- SMASThe SMAS (superficial musculoaponeurotic system) is the tissue present just underneath the skin in the face. It lies just above the parotid gland and its covering and also just above facial nerves that power the facial musculature.

The five layers of the face, analogous to layers of the scalp and neck. The facial nerve travels deep to layer 3, becoming more superficial within layer 4. (Reprinted with permission from Mendelson B. Facelift anatomy, SMAS retaining ligaments and facial spaces. In: Aston SJ, Steinbrech DS, Walden JL, eds. Aesthetic Plastic Surgery. London: Elsevier; 2009:57.)
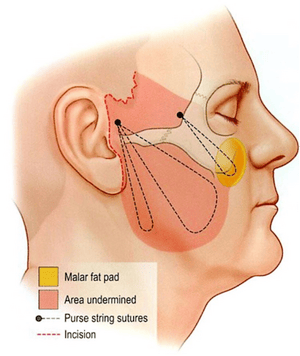
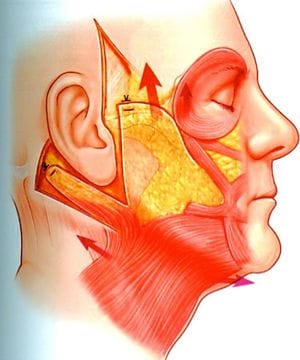
When this SMAS tissue is manipulated, the longevity of a facelift is improved. During a Mini Lift, the SMAS can be plicated, where sutures are placed to hold it up. This has been popularized with the MACS lift (Minimal Access Cranial Suspension).Illustration showing the minimal access cranial suspension lift with loop sutures tethering soft tissue to the deep temporal fascia. (Reprinted with permission from Tonnard PL, Verpaele AM, Morrison CM. MACS face lift. In: Aston SJ, Steinbrech DS, Walden JL, eds. Aesthetic Plastic Surgery. London: Elsevier; 2009:138.)
The SMAS can also be dissected from the underlying tissues forming a flap of tissue that is sutured upwards to hold facial tissues. There are proponents for both types of techniques. Although SMAS manipulation may increase the risk of nerve injury, in experienced hands, this is a rare complication.
Combining a mini-lift with SMAS manipulation is an excellent way to improve the longevity of the result. The more extensive the SMAS dissection, the more the technique starts becoming a full facelift and not a mini-lift.
Facelift
a.k.a Full Face Lift
A full facelift procedure usually involves access to the neck via a submental incision as well as the periauricular incisions. Also the dissection into the neck is more extensive than in the mini-lift variety. There are a few varieties as listed below
- Neck Dissection
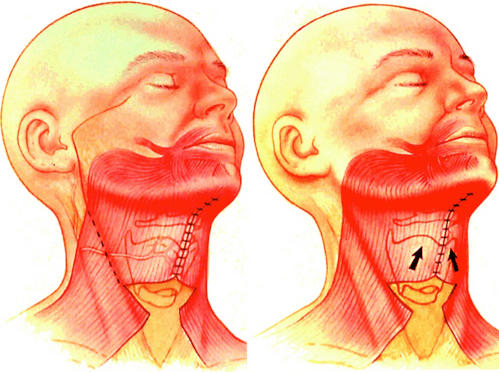
As mentioned, addressing the neck directly elevates a mini lift to a more involved face lift. A common procedure is to make a small incision under the skin dissecting over the platysmal muscles and removing excess fat. This dissection is then communicated with the dissections from each side of the face.
Medial suturing of paired platysma muscles with partial transection of the anterior border. [Reprinted with permission from Stuzin JM. MOC-PSSM CME article: Face lifting. Plast Reconstr Surg. 2008;121(1 Suppl):1–19.] - Subcutaneous FaceliftA subcutaneous facelift involves a wide undermining of skin. This is very commonly combined with manipulation of the SMAS tissues but not necessarily. A wide dissection into the neck is considered necessary to rejuvenate a very wrinkly neck.

- SMAS FaceliftThe SMAS tissues are manipulated by either suturing tissue superiorly or dissecting the tissue off the underlying tissues and then suturing it up. It is considered an important factor for improving the longevity of results

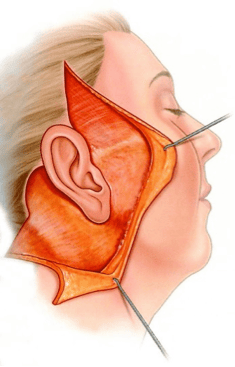
Illustration showing Barton’s “high SMAS,” with cheek soft tissue raised along with overlying skin. (Reprinted with permission from Barton FE Jr, Meade RA. The ‘HIGH SMAS’ facelift technique. In: Aston SJ, Steinbrech DS, Walden JL, eds. Aesthetic Plastic Surgery. London: Elsevier; 2009:133.) - Deep Plane or Composite FaceliftThe composite facelift involves elevation of the skin flap and the SMAS flap together in one flap. This is recommended in smokers who are at high risk for wound complications. It is technically more challenging and not used often.

Illustration showing Hamra’s original composite face lift flap, with orbicularis, malar fat, and platysma raised in continuity with overlying skin. (Reprinted from Hamra ST. Composite rhytidectomy. Plast Reconstr Surg. 1992;90:1–13.) - Subperiosteal LiftThis involves elevation of the cheek soft tissues in the subperiosteal plane. It is more of an adjunct to other techniques and helps correct cheek ptosis. It is not commonly used due to risk of an overdone appearance.
Technique of transtemporal and transbuccal subperiosteal midface lift. Reprinted from Hobar, P. C., and Flood, J. Subperiosteal rejuvenation of the midface and periorbital area: A simplified approach. Plast. Reconstr. Surg. 104: 842, 1999.